- LOGIN
- MemberShip
- 2026-07-22 03:12:20

- Company
- "Global AI drug discovery accelerates…KOR faces talent·data shortage"
- by Jung, Heung-Jun Jul 06, 2026 10:48am
- The global drug discovery ecosystem is restructuring centered on artificial intelligence (AI). Partnerships between big tech and big pharma companies are driving rapid advancements across the entire drug development lifecycle. However, the Korean biopharmaceutical industry continues to face significant hurdles, including a shortage of skilled talent and limited access to data.Dr. Pyo Junhee, Director of the AI Institute for Drug DevelopmentOn the afternoon of the 2nd, Director Pyo outlined the accelerating AI drug discovery ecosystem during a workshop titled "Future trends of AI technology in the biopharmaceutical industry," which was jointly hosted by the Pharmaceutical Society of Korea (PSK), the Korean Society of Pharmaceutical Sciences and Technology (KSPST), and the Korean Academy of FDC Regulatory Science.During her presentation, Pyo emphasized that among the pipelines currently under development by global big pharma companies, it has become difficult to find a novel drug candidate that does not integrate AI.Big pharma companies are staking its future on strengthening internal capabilities, aggressively recruiting AI engineers and data scientists for 100 to 200 positions.The growth trajectory is further accelerated by the interest and capital injection from big tech companies that view AI-driven drug discovery as a primary growth engine. Consequently, there has been a massive influx of "bio-sequence Large Language Models (LLMs)" capable of decoding and understanding biological sequences such as DNA and RNA. "Nvidia announced a partnership with Eli Lilly to build an AI drug discovery factory, while Google DeepMind developed AlphaFold3 and recently unveiled enhanced iterations of the model," Pyo explained. She noted that when Nvidia initially launched its 'BioNeMo' platform, several Big Pharma companies reportedly paused physical laboratory experiments to run toxicity predictions through BioNeMo, subsequently recalibrating their pipeline priorities. Furthermore, Anthropic recently introduced 'Claude for Science,' which offers comprehensive end-to-end workflows tailored for drug discovery. Using a multi-agent AI framework, a coordinator agent categorizes a research task, after which specialized sub-agents, focusing on genomics or structural biology, independently validate and integrate their findings.Pyo emphasized that the industry has shifted beyond merely accelerating isolated research steps. Realizing an era where hypothesis generation, experimental design, and data analysis are fully automated has already become a reality.Accordingly, Pyo stressed that the industry is no longer competing on the speed of localized workflows, but has officially entered an era of intense competition over de novo structural design.However, the Korean pharmaceutical industry continues to face bottlenecks, most notably a severe shortage of skilled personnel, as well as data scarcity and data quality issues."We conducted a survey to identify the specific pain points of domestic pharmaceutical companies and AI drug discovery firms," Pyo stated. "The most prevalent response was a shortage of proficient talent and recruitment difficulties, followed closely by data availability and quality concerns."Because proprietary drug discovery data represents a highly valuable corporate asset for individual companies, it is rarely generalized and remains highly fragmented or siloed across the industry.To address this, Pyo suggested that "data partnerships structured around commercial transactions or mutual research needs may be selectively feasible when financial incentives align. Additionally, we are seeing the emergence of specialized consortia aimed at solving common clinical goals, such as sharing control-arm data from clinical trials."The South Korean government is also actively investing in AI-driven pharmaceutical advancement through initiatives such as the K-AI Drug Discovery Preclinical and Clinical Model Development Project. In late 2025, the Ministry of Health and Welfare (MOHW) allocated approximately KRW 37.1 billion to the 'K-AI Drug Discovery Preclinical and Clinical Model Development Project', appointing lead operating organizations to foster a AI-driven development ecosystem. The Korea Pharmaceutical and Bio-Pharma Manufacturers Association (KPBMA), which houses the AIDD, was designated as a primary lead institution. "Currently, three major hospitals, pharmaceutical corporations, and research institutions are collaborating to build integrated datasets that bridge the preclinical and clinical phases," Pyo said. "Using these datasets, we are developing foundation models and a diverse array of downstream AI applications." Pyo concluded by stating, "For clinical complexities that AI alone cannot fully resolve, we are integrating various predictive simulation models to develop a platform capable of optimizing clinical trial designs."

- Opinion
- [Reporter’s View] Bio USA: Time to show results
- by Hwang, byoung woo Jul 06, 2026 10:48am
- Every year after the BIO International Convention (BIO USA) concludes, Korean biotechnology companies release a wave of press statements. They announce that they held dozens of meetings with global pharmaceutical companies, expanded partnerships, and confirmed strong interest in licensing deals for their products.However, what the market wants to know is not who they met at the conference. It wants to know how far the discussions have progressed.To be fair, the public releases are not mere publicity stunts. BIO USA remains one of the world's premier partnering events, and for Korean biotech companies, consistently participating and maintaining dialogue with global pharmaceutical companies is meaningful in itself.New drug development is not an industry where results emerge overnight. Discussions with multinational pharmaceutical companies rarely translate directly into licensing agreements. Even when negotiations are progressing well, confidentiality agreements, additional on-site inspections, data reviews, and internal decision-making processes often make it impossible to disclose developments publicly.Even so, the optimistic language that follows BIO USA each year deserves closer scrutiny. If every conference is followed by familiar phrases such as "strong global interest," "expanded partnering discussions," or "enhanced licensing opportunities," it is only natural that the market's questions shift to what comes next.More important than claiming to have attracted interest is explaining what discussions followed. More important than announcing a meeting is demonstrating whether tangible progress has been made. Whether participation in BIO USA represents a one-time event or part of a long-term business development strategy ultimately becomes evident through the company’s move after the conference.Likewise, global pharmaceutical companies evaluate far more than a company’s promising technology. They assess not only the potential of an individual pipeline candidate but also the scalability of the underlying platform, the strength of follow-on pipelines, clinical development capabilities, and the company's ability to build sustained relationships with global partners.That is precisely why continuity is highly valued in global partnering discussions.From the perspective of biotechnology companies, the situation can also be frustrating. Although the market demands rapid results, technology licensing and collaborative research agreements rarely progress on speed alone. It is not uncommon for discussions to continue for several months, or even more than a year, after an initial meeting. The absence of an immediate announcement following BIO USA does not necessarily mean the meetings produced no meaningful outcome.At the same time, however, the industry should be cautious about treating attendance itself as an achievement. Simply meeting with multinational pharmaceutical companies does not, by itself, validate a company's technological competitiveness. The number of partnering meetings held is less important than the quality of those discussions, and the real measure of success lies not in initial reactions at the conference but in subsequent validation.There is no doubt that BIO USA has helped Korean biotechnology companies strengthen their presence on the global stage. At a time when capital markets for the biotech sector remain weak, and scrutiny has intensified following technology-special listing reforms, expanding relationships with overseas partners carries significant implications for both corporate value and long-term survival. Dialogue with multinational pharmaceutical companies can also help companies better understand the competitiveness of their technologies and refine future development directions.However, the industry has now reached a point where results must accumulate alongside the rhetoric. It is time to ask whether ‘expanded discussions’ led to additional meetings, whether ‘strong interest’ resulted in requests for data or joint evaluations, and whether ‘strengthened partnerships’ evolved into lasting relationships that continue at later conferences.BIO USA is an annual event. That is precisely why the venue is important. More important than participating once is demonstrating more mature data the following year, continuing deeper discussions with the same partners, and ultimately delivering on the commitments made to the market. The company’s true success from BIO USA is realized only after the event concludes.
- Policy
- Generic reimb listings jump 24% in 1H ahead of pricing ratio cut
- by Jung, Heung-Jun Jul 06, 2026 10:48am
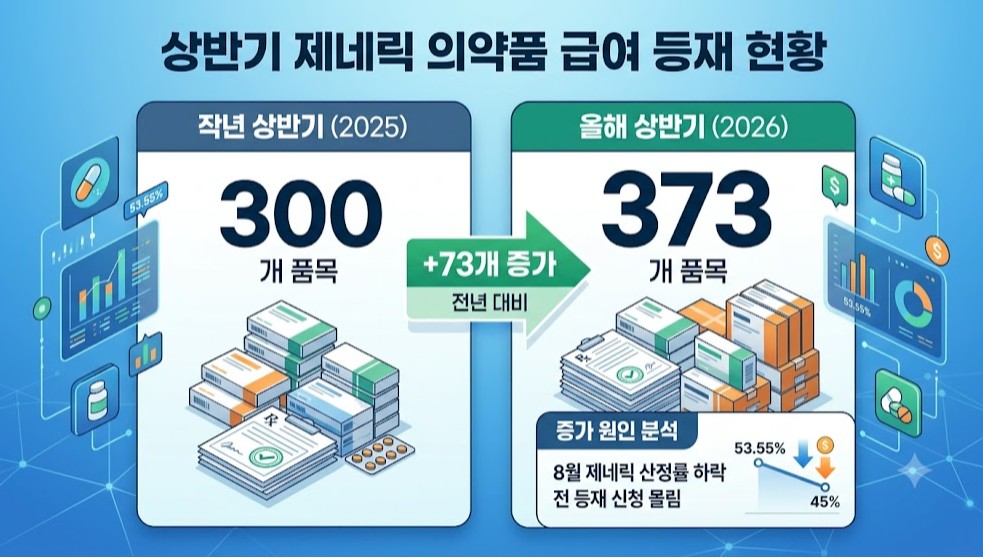
- The number of generic drugs added to Korea's National Health Insurance reimbursement list increased 24% YoY in the first half of 2026. Industry experts view this rise as the pharmaceutical companies’ rush to secure reimbursement listings ahead of the scheduled reduction in the generic pricing ratio to 45% in August.According to health authorities and industry sources on July 3, a total of 373 generic products were added to the reimbursement list between January and June this year.AI-generated imageBy comparison, 300 generic products were listed during the same period last year, meaning 73 more products entered the reimbursement list in the first half of 2026.However, the increase cannot be attributed solely to the upcoming pricing reform and the rate reduction that is set to follow. Reimbursement applications also tend to surge when patents or post-marketing surveillance (PMS) exclusivity for major products expire.For example, following the expiration of the compound patent for Jardiance in October last year, 235 follow-on generics from 37 pharmaceutical companies were simultaneously added to the reimbursement list.Given that no major products lost patent or PMS protection during the first half of this year, the industry believes the government's pharmaceutical pricing reform played a significant role in the increase.The pricing reform announced in November last year included a substantial reduction in the generic reimbursement pricing ratio from the original 53.55%. For companies that are not designated as innovative or quasi-innovative pharmaceutical manufacturers, the lower pricing ratio is expected to significantly reduce reimbursement prices and directly affect product sales.In addition, the penalty for failing to satisfy all reimbursement eligibility criteria will increase from 15% to 20%, further encouraging companies to obtain reimbursement listings before the revised pricing rules take effect.Including the 69 generic products added to the reimbursement list this month, a total of 442 generic products have newly gained reimbursement coverage this year. These products effectively represent the final group to secure reimbursement before the pricing rate is lowered next month.In May, the Ministry of Health and Welfare (MOHW) released proposed revisions to the ‘Standards for the Determination and Adjustment of Drug Prices’ for public comment, with the consultation period remaining open until July 13.The revised notification is scheduled to take effect on August 1. From that date, the generic pricing ratio will be reduced from 53.55% to 45%.Under the revised framework, generic products meeting all reimbursement eligibility criteria will receive a pricing ratio of 45%, those satisfying one criterion will receive 36%, and products meeting none of the criteria will be priced at 29% of the reference level.
- Policy
- Talks continue on price cuts for listed fixed-dose combos
- by Jung, Heung-Jun Jul 06, 2026 10:48am
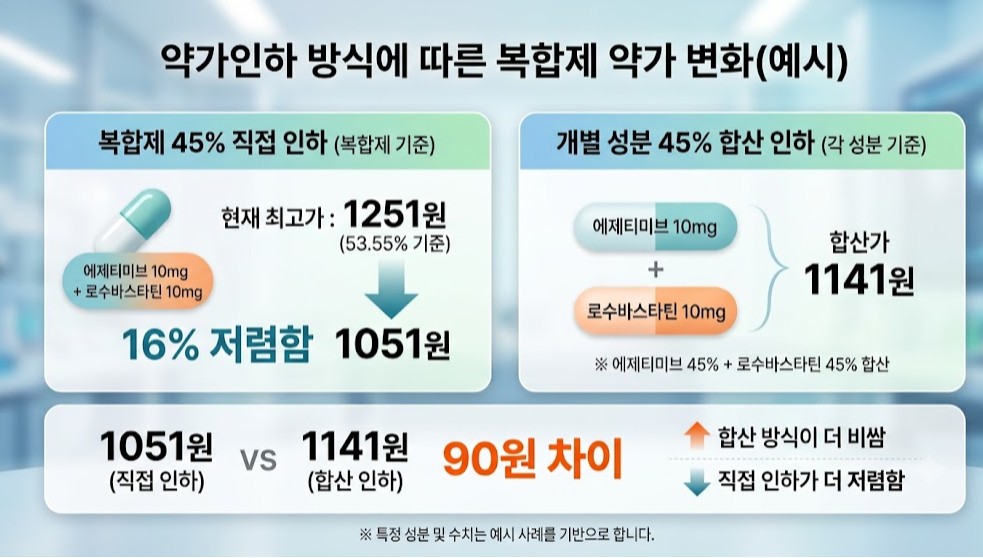
- With follow-up working-level discussions on price reductions for already-listed fixed-dose combination (FDC) products set to continue, reimbursement prices for FDCs are at risk of being uniformly cut, with the extent depending on the final pricing formula.If the government applies the 45% cut rate to the current maximum reimbursement level for FDCs, set at 53.55%, FDC prices would be reduced by approximately 16%, mirroring the across-the-board reduction planned for single-ingredient products.As a result, the pharmaceutical industry is expected to propose an alternative approach under which FDC reimbursement prices would be calculated by summing the reimbursement prices of each ingredient after applying the 45% pricing ratio.According to industry sources on July 6, the Ministry of Health and Welfare (MOHW), the Health Insurance Review and Assessment Service (HIRA), the National Health Insurance Service (NHIS), and industry representatives will hold another working-level meeting on the drug pricing reform, with price reductions for listed FDC products set to be one of the key agenda items.With the revised ‘Standards for the Determination and Adjustment of Drug Prices’ scheduled to take effect next month and the implementation of price reductions for listed products to follow, the government is expected to finalize the methodology for reducing reimbursement prices of FDC products soon.During previous discussions, using the current maximum reimbursement level for FDCs (53.55%) as the baseline and recalculating prices using the new 45% pricing ratio was proposed.AI-generated imageThe pharmaceutical industry, however, has consistently pushed for FDC reimbursement prices being set by adding together the revised reimbursement prices of each individual ingredient after applying the 45% pricing ratio separately.For example, an ezetimibe 10 mg/rosuvastatin 10 mg fixed-dose combination currently has a maximum reimbursement price of KRW 1,251. If that price is deemed to be 53.55% and recalculated directly to 45%, the reimbursement price would fall by approximately 16% to KRW 1,051. In contrast, if the reimbursement prices of ezetimibe 10 mg and rosuvastatin 10 mg are each recalculated at 45% and then combined, the resulting reimbursement price would be KRW 1,141, representing a smaller reduction of approximately 8.8%.Because reimbursement price reductions are directly linked to declines in product revenue, the industry naturally favors the latter methodology, combining the reimbursement prices of the individual components.Industry stakeholders also argue that the current reimbursement system already affects FDC prices through changes in the reimbursement prices of their individual components and contend that the same linkage principle should also be applied when implementing price reductions for listed FDC products.If the individual 45% pricing approach is adopted, the extent of the price reduction would vary depending on the specific dosage combination. Some products could see only minimal price decreases, allowing manufacturers to partially offset the expected decline in sales.However, the government has maintained its position that FDC products should be subject to the same uniform 16% reduction as single-ingredient products. Consequently, it is considered unlikely that authorities will accept the industry's proposal to base reimbursement prices on the combined reimbursement levels of the individual components.
- Company
- 'Perjeta' adjuvant therapy resubmitted to the CDRC
- by Eo, Yun-Ho Jul 06, 2026 10:48am
- Product photo of PerjetaAttention is focused on whether the post-operative adjuvant therapy indication for breast cancer treatment, 'Perjeta,' can be revived in the market.According to industry sources, an application for the expanded reimbursement criteria for the post-operative adjuvant therapy of Roche Korea's HER2-positive breast cancer treatment Perjeta (pertuzumab) is scheduled to be considered at the upcoming meeting of the Cancer Disease Review Committee (CDRC) of the Health Insurance Review and Assessment Service (HIRA) on the 8th.Earlier this year, the Breast Cancer Division of the Korean Society of Medical Oncology (KSMO) submitted its application to expand the reimbursement criteria for Perjeta. While a prior expansion request by Roche was expected to be reviewed by the CDRC in October last year, the discussion fell through due to a regulatory realignment of the selective reimbursement criteria for pharmaceuticals.Currently, Perjeta is reimbursed for HER2-positive metastatic or unresectable locally recurrent breast cancer. For early-stage breast cancer, it is reimbursed under selective reimbursement as a neoadjuvant/pre-operative therapy, with a patient co-payment rate of 30%.However, its use as a post-operative adjuvant therapy, a critical therapeutic stage for preventing disease recurrence, has remained non-reimbursed (100% out-of-pocket patient cost) since regulatory approval in South Korea in 2018, thereby limiting patient access.Unlike the neoadjuvant chemotherapy, which is reimbursed under the 30% selective reimbursement, the adjuvant indication lacked high-level recommendation grades in global clinical guidelines or long-term follow-up data at the time of its initial review in 2019.However, the 10-year follow-up results from the global Phase 3 APHINITY trial, published last year, are anticipated to fill this clinical evidence gap.According to the study, the adjuvant combination therapy of Perjeta + 'Herceptin (trastuzumab)' demonstrated a clear clinical benefit, significantly reducing the risk of death by 21% compared to monotherapy in the lymph node-positive patient cohort, who face a high risk of disease recurrence.Meanwhile, the Perjeta-Herceptin combination therapy is currently recommended as a Category 1 treatment under the U.S. NCCN Guidelines for post-operative adjuvant therapy in lymph node-positive, HER2-positive early breast cancer. It is being recommended a Category 1 recommendation for post-operative adjuvant therapy in high-risk, lymph node-positive patients who have achieved a pathological complete response (pCR) following neoadjuvant chemotherapy.
- Opinion
- "Shifting hypertension management…'indapamide'-based triple comb"
- by Son, Hyung Min Jul 03, 2026 09:03am
- The standard of care in hypertension treatment is shifting.The recently announced 2026 Guidelines for Hypertension have strengthened target blood pressure goals to below 130/80 mmHg for high-risk cardiovascular patient populations while actively recommending the implementation of upfront combination therapies. As achieving these blood pressure targets relies heavily on dual and triple regimens alongside Single-Pill Combinations (SPCs), changes to treatment strategies are anticipated.Professor Kwang-il Kim of the Department of Geriatric Medicine at Seoul National University Bundang HospitalThis revision expands beyond a simple numeric adjustment of blood pressure targets. Its significance lies in integrating proactive blood pressure-lowering strategies validated by recent landmark clinical trials, including STEP, ESPRIT, and BPROAD. These studies confirmed that intensive blood pressure control directly correlates with a reduced risk of major cardiovascular and cerebrovascular events and mortality.According to the revision, the target blood pressure for hypertensive patients with concomitant diabetes has been systematically lowered to below 130/80 mmHg. Similarly, for patients with chronic kidney disease (CKD), a strict target below 130/80 mmHg is now recommended regardless of proteinuria status, with instructions to consider a systolic blood pressure (SBP) target below 120 mmHg if tolerated by the patient. Furthermore, the SBP target for patients with a history of stroke has been intensified from the conventional threshold of below 140 mmHg to below 130 mmHg.In contrast, the target blood pressure for elderly hypertensive patients and general patients presenting with uncomplicated hypertension remains at the previous threshold of below 140/90 mmHg. This differentiation reflects clinical evidence showing clear prognostic benefits from aggressive blood pressure reduction in high-risk cohorts, contrasted against insufficient data supporting additional clinical benefits for intensive lowering in low-to-moderate risk populations.Professor Kwang-il Kim of the Department of Geriatric Medicine at Seoul National University Bundang Hospital, who also serves as the Chairman of the Korean Society of Hypertension, discussed these shifting paradigms. During a meeting with DailyPharm, Kim said, "Managing systolic blood pressure down to 130 mmHg is significantly different from managing to 140", and added, "Because target blood pressure metrics have lowered, patients will likely require the addition of one or more therapeutic intervention, requiring active treatment."Professor Kim emphasized that "Lowering blood pressure targets in high-risk patient populations is not merely shifting metrics, but a foundational clinical approach to reducing overall cardiovascular event risk and improving long-term prognosis."Early intervention using second-line treatment is highlightedHypertension remains a primary risk factor driving critical cardiovascular sequelae, including myocardial infarction, stroke, heart failure, and chronic kidney disease. For patients with preexisting metabolic or structural comorbidities like diabetes, CKD, or a history of cardiovascular events, even marginal elevations in baseline blood pressure can exponentially increase the risk of an acute cardiovascular event, necessitating rigid clinical control. Consequently, the updated guidelines indicate the importance of early use of combination therapy alongside tighter blood pressure targets.Previously, standard clinical practice followed a stepped-care approach, initiating monotherapy and only escalating dosages or adding secondary classes if a patient failed to achieve target ranges. However, real-world clinical environments have long struggled with therapeutic inertia, where physicians fail to intensify treatment regimens despite patients missing their therapeutic targets. This has been criticized as a major barrier to improving blood pressure control rates.Professor Kim explained, "Clinical tendencies among healthcare providers and patient medication adherence represent are the primary reasons for blood pressure control failure," and added, "To rapidly achieve and sustainably maintain target blood pressure over long-term timelines, initiating appropriate combination therapies early in the treatment algorithm is essential, adding that deploying these regimens as fixed-dose SPCs is highly preferable."To support the clinical adoption of SPCs, the 2026 guidelines have introduced a modernized classification framework that categorizes these formulations into ultra-low-, low-, standard-, and high-dose combinations. The Korean Society of Hypertension formally positions SPCs as therapeutically superior to loose-dose multi-pill combinations, particularly in terms of blood pressure reduction rates and long-term treatment persistence.Professor Kim highlighted that South Korea possesses a distinct competitive advantage given its highly developed pipeline of diverse SPC formulations and dosage configurations, noting that this wide selection significantly enhances prescribing flexibility for clinicians.Guidelines introduced the category of intractable hypertension…has expanded the importance of triple combination therapyThe updated guidelines have also newly introduced the diagnostic and therapeutic approach for patients presenting with difficult-to-treat hypertension.Most notably, the guidelines have officially introduced the clinical definition of 'intractable hypertension,' expanding upon the traditional concept of resistant hypertension. Intractable hypertension classifies cases where patients fail to reach their target blood pressure goals despite the concurrent utilization of two or more antihypertensive drug classes, including a mandatory diuretic component. This expanded categorization integrates both resistant and refractory hypertension, thereby establishing more systematic diagnostic and therapeutic algorithms in real-world clinical practice.When intractable hypertension is suspected, the guidelines advise clinicians against blindly escalating pill burdens. Instead, providers are directed to first verify patient medication compliance and validate the accuracy of blood pressure measurements. Clinicians must rule out white-coat hypertension by using home blood pressure monitoring (HBPM) or ambulatory blood pressure monitoring (ABPM), while thoroughly evaluating secondary hypertension etiologies, lifestyle factors, and concomitant medications that may inadvertently elevate blood pressure.Professor Kim emphasized that "Unadjusted high blood pressure readings do not automatically indicate absolute drug resistance," and added, "Poor compliance, measurement errors, or white-coat effects frequently skew clinical metrics." "Once these confounding variables are resolved, a more intensive pharmacotherapeutic strategy must be applied to patients who remain uncontrolled."Specifically, the guidelines highlight the therapeutic importance of a triple combination regimen anchored by an ACE inhibitor or Angiotensin Receptor Blocker (ARB), a Calcium Channel Blocker (CCB), and a diuretic.Because the pathogenesis of hypertension involves multifaceted, overlapping systems, such as renin-angiotensin system activation, peripheral vasoconstriction, and volume expansion, a triple combination addressing these separate pathways simultaneously is recognized as a highly effective clinical strategy.Professor Kim stated, "Targeting a single physiological pathway rarely yields sufficient blood pressure lowering," and added, "Transitioning to triple combination therapy may be a highly efficient approach when dual combination therapies fail." "The clinical importance of triple combination therapy will expand significantly as high-risk patients require additional agents to meet tighter blood pressure targets," Professor Kim added.Industry focuses on indapamide-based triple combination therapiesIn line with these shifting treatment environments, diverse triple combination therapies are being introduced to the domestic market. Indapamide-based triple combination therapies, such as Ankook Pharmaceutical’s 'Levosartan Plus' (a fixed-dose combination of valsartan, S-amlodipine, and indapamide), are attracting significant industry attention amid the clinical push for tighter blood pressure goals and expanded SPC utility.Indapamide is recognized not only for its diuretic effect, which reduces fluid volume, but also for its direct vasodilatory properties. As a representative thiazide-like diuretic, it has a long-established clinical history, demonstrating blood pressure-lowering efficacy and a favorable metabolic safety profile.Professor Kim said, "Long-term cardiovascular prognostic benefits have been firmly established for thiazide-like diuretics like indapamide and chlorthalidone across landmark clinical trials, including the HYVET study," and added, "Indapamide offers a distinct clinical advantage due to its minimized risk of metabolic adverse events."Global guidelines similarly recommend prioritizing thiazide-like diuretics over conventional thiazide diuretics. S-amlodipine is attracting clinical interest in light of the updated guidelines. Professor Kim suggested that switching to S-amlodipine represents a viable therapeutic strategy for patients experiencing CCB-induced side effects, such as peripheral edema.Professor Kim suggested that "S-amlodipine maintains robust blood pressure lowering efficacy while significantly reducing the incidence of peripheral edema compared to conventional amlodipine," and added, "It could be a major alternative for patients whose medication adherence drops due to swelling."Professor Kim concluded by stating, "Valsartan is an ARB with extensive prognostic evidence, and indapamide is a clinically proven thiazide-like diuretic," and added, "This combination represents a highly effective, optimized therapeutic option for high-risk patients requiring intensive blood pressure reduction."
- Company
- MSD-Boryung signs copromotion agreement for Enflonsia
- by Kim, Jin-Gu Jul 03, 2026 09:03am
- MSD Korea has partnered with Boryung Biopharma to commercialize Enflonsia (clesrovimab), its monoclonal antibody for the prevention of respiratory syncytial virus (RSV) in neonates and infants.According to industry sources, on July 1 the two companies signed a strategic partnership agreement covering domestic distribution and co-promotion of Enflonsia in Korea. Under the agreement, Boryung Biopharma will begin handling domestic distribution and joint promotional activities targeting healthcare professionals starting July 1.Enflonsia is a long-acting monoclonal antibody that provides at least 5-6 months of protection following a single dose in neonates and infants. In the large-scale global Phase III CLEVER trial, the therapy demonstrated clinical efficacy, reducing RSV-related hospitalizations by 84.2%.Expectations are rising on site on the convenience of administration of Enflonsia. Compared with Beyfortus, which has already established a presence in the market, Enflonsia offers a simpler dosing regimen. Beyfortus requires different dosage strengths depending on an infant's body weight (5 kg) as the dosing threshold. In contrast, Enflonsia is administered as a single fixed dose regardless of body weight.The infant RSV prevention market in Korea is currently led by Sanofi and SK Bioscience. To strengthen its market position, MSD Korea selected Boryung Biopharma as its commercialization partner, citing the company's extensive distribution network and long-standing expertise in vaccine and pharmaceutical sales, particularly in primary care clinics.The upcoming RSV season in the second half of the year is expected to be the first major commercial opportunity for Enflonsia. In Korea, the RSV season typically runs from October through March. Infants born during the RSV season are expected to receive a single dose shortly after birth, while those born outside the season are scheduled to receive one dose before the start of their first RSV season. The two companies plan to rapidly expand the product's market presence in line with this schedule.Although RSV infection typically begins with symptoms resembling those of the common cold, it can progress to lower respiratory tract infections, including bronchiolitis and pneumonia, in infants younger than one year of age, often requiring hospitalization.According to a nationwide study based on National Health Insurance claims data covering 2007 to 2019, published last year, 44.7% of Korean children younger than five years diagnosed with RSV required hospitalization. In particular, infants aged 6 to 11 months accounted for approximately 48.2% of RSV-related hospitalizations and 57.3% of intensive care unit (ICU) admissions among children under five, representing the highest hospitalization burden. Infants younger than six months had the longest average hospital stay, at 8.35 days.Enflonsia received marketing authorization in Korea on July 1. The approval was supported by results from the global Phase IIb/III CLEVER trial and the Phase III SMART study.The CLEVER study evaluated approximately 3,600 healthy newborns and infants born at 29 weeks' gestation or later across 22 countries and demonstrated a 60.4% reduction versus placebo in the primary endpoint of medically attended lower respiratory tract infection (MALRI) associated with RSV.In the safety analysis, more than 96% of adverse events reported with Enflonsia were mild or moderate in severity. The Phase III SMART study, which enrolled premature infants and infants at high risk for severe RSV disease, including those with chronic lung disease (CLD) or congenital heart disease (CHD), also demonstrated an overall safety profile comparable to that of the control treatment (palivizumab).

- Company
- Nature highlights Hanmi, SK Biopharm’s innovation
- by Cha, Ji-Hyun Jul 03, 2026 09:03am
- The global pharmaceutical and biotechnology industry is increasingly recognizing the growing presence of K-Bios. A leading international journal in drug discovery has identified Hanmi Pharmaceutical and SK Biopharmaceuticals as companies leading the development of innovative medicines among biopharmaceutical firms in Asia and other emerging markets, highlighting Korea's transition from a generic-focused industry to one driven by research and development (R&D)-based innovation-driven new drug porfolio.According to the Korea Biotechnology Industry Organization's Bioeconomy Research Center on July 2, ‘Nature Reviews Drug Discovery’ recently published an analysis examining changes in R&D productivity among biopharmaceutical companies across Asia and emerging markets. Nature Reviews Drug Discovery is one of the most prestigious publications in drug discovery and development. It had a 2024 Journal Impact Factor (JIF) of 101.8, placing it among the world's highest-impact scientific journals.The researchers evaluated 45 biopharmaceutical companies with annual sales exceeding USD 500 million over the 2010–2025 period. The analysis assessed R&D investment, clinical pipeline composition, and revenue trends to determine the extent to which each company had transitioned from a generic-based business model to an innovation-driven new drug portfolio. Companies were subsequently classified as innovation leaders, emerging innovators, or generic-focused companies based on their R&D intensity and proportion of innovative assets.Among Korean companies, Hanmi Pharmaceutical and SK Biopharmaceuticals were classified as innovation leaders, the highest category in the study. They joined 9 Chinese companies in the same group, including BeOne, CSPC Pharmaceutical Group, Jiangsu Hengrui Pharmaceuticals, Henlius, Innovent Biologics, Junshi Biosciences, and Sino Biopharmaceutical. The findings place the two Korean companies alongside some of China's leading global pharmaceutical firms.Hanmi Pharmaceutical was recognized for maintaining a consistently high level of R&D investment. According to the study, the company invested approximately 17% of its revenue in R&D over the past decade, up from roughly 10% during the 2010–2015 period. The journal also highlighted Hanmi's strategy of focusing on innovative drug development in metabolic and rare diseases.Hanmi is currently expanding its pipeline, particularly in obesity and metabolic disorders. Its long-acting GLP-1 (glucagon-like peptide-1) obesity candidate efpeglenatide, developed using the company's proprietary ‘LAPSCOVERY’ platform, has advanced into the regulatory submission stage based on positive domestic Phase III results. The company is also broadening its metabolic disease portfolio by developing a GLP-1/GIP/glucagon triple agonist and next-generation obesity therapies designed to preserve and increase muscle mass. In addition, Hanmi continues to develop novel therapies for rare diseases and oncology using its proprietary technology platforms.Analysis of R&D Intensity and Portfolio Innovation Index Across 45 Biopharmaceutical Companies in Asia and Emerging Markets (2010–2025), Published in the International Journal Nature Reviews Drug Discovery (Source: Bioeconomy Research Center, KoreaBIO)The published analysis also recognized SK Biopharmaceuticals as an innovation leader, reflecting its successful development and global commercialization of proprietary medicines. The company has established a fully integrated business model spanning drug discovery through commercialization, with a focus on central nervous system (CNS) disorders.SK Biopharmaceuticals is expanding into next-generation therapeutic modalities, building on the global development and commercialization experience gained through its proprietary epilepsy drug ‘cenobamate.’ In addition to its CNS franchise, the company has identified radiopharmaceutical therapy (RPT) and targeted protein degradation (TPD) as future growth engines. It is currently developing multiple radiopharmaceutical candidates based on actinium-225 and lutetium-177, while also advancing oncology programs utilizing TPD technology.유한양행, 대웅제약, 삼성바이오로직스, GC는 신흥 혁신기업에 이름을 올렸다. 연구진은 이들 기업을 혁신 선도기업 단계로 분류하지는 않았으나 제네릭 중심 기업과 달리 R&D 투자와 혁신 포트폴리오 전환을 이어가는 기업군으로 평가했다.Yuhan Corporation, Daewoong Pharmaceutical, Samsung Biologics, and GC were classified as emerging innovators. Although they were not placed in the innovation leader category, the researchers recognized these companies as actively increasing R&D investment and shifting toward innovation-based portfolios rather than relying primarily on generic medicines.In particular, Yuhan Corporation’s R&D spending rose from less than 5% of revenue during 2010–2015 to approximately 12% during 2020–2025. Its growing investment in oncology research and its strategic transition from a traditional generic-based business to an innovation-focused pharmaceutical company were cited as key factors behind its classification.The findings carry significance as it signifies that the structural transformation of Korea's pharmaceutical and biotechnology industry is now gaining recognition on the global stage. Korean companies have steadily demonstrated their innovative capabilities through technology licensing, global clinical development, and overseas approvals of proprietary medicines. The findings published this time are noteworthy because it attributes these achievements not to isolated successes by individual companies, but to sustained increases in R&D investment and a long-term shift toward innovation-driven portfolios.The researchers concluded, "Several leading biopharmaceutical innovators in Asia, particularly those in China and South Korea, have chosen the path of innovation and are well positioned to challenge established global competitors in Europe and the United States over the coming years."
- Company
- Breztri enters reimbursement price negotiations
- by Eo, Yun-Ho Jul 03, 2026 09:02am
- The triple-combination inhaler ‘Breztri’ has entered the final stage of the National Health Insurance reimbursement process in Korea.According to industry sources, the Ministry of Health and Welfare (MOHW) recently instructed the National Health Insurance Service (NHIS) to begin reimbursement price negotiations for Breztri Aerosphere (budesonide/glycopyrronium/formoterol), which is marketed by AstraZeneca Korea for the maintenance treatment of adults with moderate to severe COPD. The first round of negotiations is expected to begin next week.Breztri entered price negotiations after agreeing to receive a price below the price assessed as appropriate by the Drug Reimbursement Evaluation Committee (DREC) of the Health Insurance Review and Assessment Service (HIRA) in May.Breztri Aerosphere is a single-inhaler triple therapy (SITT) combining an inhaled corticosteroid (ICS), a long-acting β2-agonist (LABA) and a long-acting muscarinic antagonist (LAMA) in one inhaler. It is indicated as maintenance therapy for adults with COPD to improve symptom control and reduce exacerbations, and is administered twice daily.The efficacy and safety of Breztri Aerosphere have been confirmed in the global Phase III ETHOS and KRONOS trials.The ETHOS (The Efficacy and Safety of Triple Therapy in Obstructive Lung Disease) study was a multicenter, randomized, double-blind Phase III trial involving 8,588 patients (aged 40 to 80 years) with moderate to very severe COPD who were treated over 52 weeks.Study results showed that Breztri Aerosphere reduced the annual rate of moderate or severe COPD exacerbations by approximately 24% compared with LAMA/LABA dual therapy, and by approximately 13% compared with ICS/LABA therapy, with both differences reaching statistical significance.In a post hoc analysis of the ETHOS study, treatment with Breztri Aerosphere was also associated with a significant reduction in all-cause mortality compared with LAMA/LABA therapy.Another pivotal Phase III trial, KRONOS, demonstrated improvements in lung function with Breztri Aerosphere.The KRONOS study enrolled 1,902 patients with moderate to very severe COPD and followed them for 24 weeks. At Week 24, Breztri Aerosphere improved lung function by 22 mL compared with LAMA/LABA therapy and by 74 mL compared with ICS/LABA (BFF MDI).COPD is a representative chronic respiratory disease caused by abnormalities of the airways and alveoli, including chronic bronchitis, bronchiolitis, and emphysema. It is characterized by chronic respiratory symptoms such as dyspnea and cough, together with persistent and progressive airflow obstruction.According to the 2026 Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines, triple therapy with ICS, LAMA and LABA is recommended for patients receiving ICS/LABA who either continue to experience a high symptom burden despite no recent exacerbations or who experience exacerbations with a blood eosinophil count of at least 100 cells/μL.
- Policy
- Novo Nordisk's hemophilia A treatment 'denecimig' wins ODD
- by Lee, Tak-Sun Jul 02, 2026 09:17am
- AI-generated imageNovo Nordisk's hemophilia A treatment 'denecimig (injection)' and Novartis's 'ianalumab (injection)' for moderate-to-severe adult Sjögren's disease have been designated as orphan drugs.On the 1st, the Ministry of Food and Drug Safety (MFDS) officially announced these new designations. Through this revision, both ingredients have been officially listed on the orphan drug list under Item Ga (Table 1) and Item Na (Table 2) of Article 2, Subparagraph 18 of the Pharmaceutical Affairs Act, respectively, providing novel therapeutic alternatives in the rare disease market in South Korea.First, 'denecimig (injection)', added as the 8th ingredient under Item Ga (Table 1) of the Pharmaceutical Affairs Act, is a novel candidate being developed by Novo Nordisk to address hemophilia A, a prominent rare hemorrhagic disorder. Under current domestic regulations, 'Item Ga' classifications are reserved for therapies targeting rare conditions officially designated by the Ministry of Health and Welfare (MOHW) under the 'Rare Disease Management Act'. The regulatory inclusion of denecimig is expected to significantly broaden clinical choices for domestic hemophilia A patients who face a lifelong risk of spontaneous hemorrhage and subsequent articular complications.The inclusion of denecimig expands Item Ga (Table 1) orphan drug list of the MFDS comprising eight active ingredients. The current Item Ga list already includes 'nipocalimab (injection)' for generalized myasthenia gravis, which causes systemic muscle weakness; 'pegunigalsidase alfa (injection)' for Fabry disease, a disorder where intracellular glycolipid accumulation leads to renal and cardiac impairment; and 'onasemnogene abeparvovec (injection)' for infantile, pediatric, bulbar, and adult-onset spinal muscular atrophy (SMA), which induces muscle wasting via motor neuron degeneration.The list has been expanded to include eight items, including 'garadacimab (injection)' for C1-esterase inhibitor deficiency, which triggers acute subcutaneous and mucosal edema; 'miglustat (capsule)' and 'cipaglucosidase alfa (injection)' administered in combination for Pompe disease, which causes progressive muscle weakness; 'vamorolone (oral suspension)' for severe muscular dystrophy, a pediatric genetic disorder characterized by progressive muscle loss; and 'acoramidis hydrochloride (tablet)' for transthyretin amyloid cardiomyopathy (ATTR-CM), where abnormal amyloid fibril deposition leads to heart failure, alongside the newly added hemophilia A treatment denecimig (injection).Additionally, 'ianalumab (injection)', listed under No. 409 in Item Na (Table 2) of the Pharmaceutical Affairs Act, was developed by Novartis as a treatment for patients with moderate-to-severe adult Sjögren's disease. The "Item Na" designation is granted to medicinal products targeting diseases with a domestic prevalence of 20,000 or fewer individuals, where no appropriate alternative treatment is available or where the candidate demonstrates a significantly improved safety or efficacy profile compared to existing standards of care.Sjögren's disease is a systemic autoimmune disorder characterized by chronic exocrine gland inflammation accompanied by severe dry eyes, dry mouth, and arthralgia. Yet, there has been a significant unmet medical need due to the absence of targeted, disease-modifying therapies. As a monoclonal antibody injection, ianalumab targets and inhibits B cells driving the autoimmune response, anticipated to mark a significant turning point for patients who previously lacked viable therapeutic options.An MFDS official said, "This revision is a measure to provide safe and effective therapeutic options for patients with hemophilia A and Sjögren's disease, who have faced hardships due to limited local patient populations or a lack of alternative treatments. The official added that the ministry will continue to actively use the Item Ga and Na system to enhance patient access to treatments for rare and intractable conditions, while rapidly designating essential medicines to establish a stable domestic supply chain.Once an item is designated as an orphan drug, it becomes eligible for expedited review during the marketing authorization process. It receives various commercial and regulatory incentives, including a specified period of post-marketing exclusivity. Furthermore, the submission requirements for regulatory approval are streamlined, enabling pathways such as conditional approval and waivers for local bridging data, and an expedited evaluation process is implemented through priority review. Additionally, reductions or exemptions of regulatory application fees are provided.