- LOGIN
- MemberShip
- 2026-06-18 12:14:12
- How to address the growing backlog of non-reimbursed therapies
- by Son, Hyung Min | translator Alice Kang | 2026-06-17 16:30:59

So, is there a solution? The reality that the number of non-reimbursable anticancer drugs is piling up as advanced new drugs increase is causing frustration for patients.
However, the regulatory authorities also have their woes, as the faster innovative cancer therapies are developed, the greater the burden placed on Korea's National Health Insurance system.
With the introduction of new classes of oncology treatments, including immunotherapies, antibody-drug conjugates (ADCs), bispecific antibodies, radiopharmaceuticals, and gene therapies, cancer survival outcomes have steadily improved. In some cancers, discussions have progressed beyond long-term survival to the possibility of a cure. For the National Health Insurance Service, however, the advances have come with rapidly increasing financial pressure as treatment costs often reach hundreds of thousands of dollars per patient.
The core problem is that Korea's reimbursement system has struggled to keep pace with the speed of drug development and regulatory approval. Even therapies that have become global standards of care often require years to obtain reimbursement, leaving patients waiting long after approval until they can actually benefit from treatment.
According to the Korea Alliance of Patients Organization, the average time from regulatory approval to reimbursement listing for 32 oncology drugs listed between 2021 and 2025 was 659 days, which is approximately 1 year and 10 months.
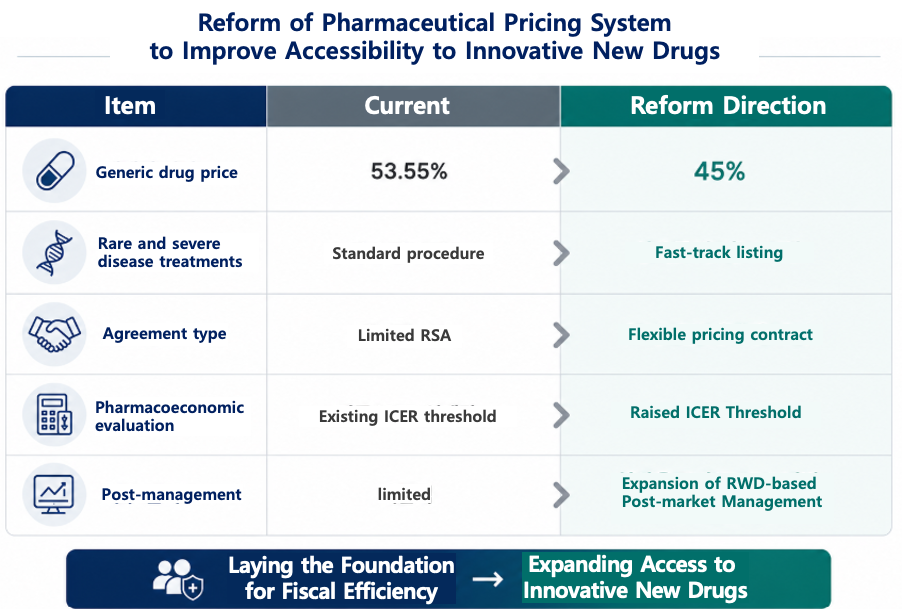
Against this backdrop, attention is rising on whether the government's ongoing drug-pricing reform could provide part of the solution. The government ultimately plans to improve patient access to innovative medicines through the generic drug pricing reform, which includes measures to improve financial efficiency, accelerate reimbursement for rare-disease and severe-disease treatments, introduce flexible pricing agreements, and expand risk-sharing agreements.
"It's not just about money, it's about value"…Consensus forms on the need to change the reimbursement evaluation system
The medical community criticized that reimbursement decisions for cancer drugs should not be viewed solely as financial issues. However, clinicians continue to believe that budget impact remains one of the most influential variables in reimbursement decisions.
One medical oncologist commented, “In many recent reimbursement reviews, projected claims amount seems to carry more weight than treatment effectiveness. Particularly in cancers that affect many patients, reimbursement discussions can drag on simply because of the anticipated financial burden, regardless of how strong the clinical benefit may be."
"Paradoxically, the more patients who could benefit from a treatment, the harder it sometimes becomes to obtain reimbursement. Even therapies with proven survival benefits may face access barriers because of financial concerns."
One expert involved in CDRC discussions described the reimbursement process as “not a process of calculating costs, but a process of putting a price tag on value."
According to the expert, "Cost-effectiveness is not simply about whether a drug is expensive or inexpensive. It is about determining how much society is willing to pay for extended survival, improved quality of life, and the possibility of a cure. Although discussions are made using Korea’s per-capita GDP of approximately USD 36,000 as a benchmark, for severe diseases and oncology treatments, society may need to consider doubled thresholds, those exceeding USD 70,000.
“Below USD 36,000, treatments are generally viewed as more acceptable, and the burden becomes much greater when the threshold exceeds USD 70,000. Between those levels, the question is ultimately about which values society chooses to prioritize. That is less a scientific judgment than a social choice."
There are also growing calls for improving the predictability and transparency of the current reimbursement evaluation system. At present, the results of the Cancer Disease Deliberation Committee (CDDC) are disclosed in forms such as reimbursement criteria established, reimbursement criteria not established, or reconsideration. However, it is not possible to determine which specific factors influenced the decision.
One pharmaceutical industry official said, “Only the result -- ‘reimbursement criteria not established’ -- is disclosed, so it is difficult to determine whether the decision was due to insufficient clinical evidence, cost-effectiveness issues, or budget impact. From a company’s perspective, it is not easy to predict what needs to be supplemented in order to expect a positive outcome at the next review.”
The official continued, “We agree that reimbursement evaluation is a process of finding a balance between financial sustainability and patient access. If there is insufficient explanation of the decision-making process, acceptance of the outcome may also be reduced. There is also a need for discussions on sharing evaluation criteria and the rationale behind making decisions more transparently.”
Generic drug pricing reform… Whether the cost savings are reinvested in innovative drugs is key
The drug pricing system reform being pursued by the government can also be viewed as part of the search for an answer to the same question. If the financial resources secured through generic drug price cuts lead to improved access to innovative medicines, and if the reimbursement system becomes able to reflect treatment value more flexibly, this reform could become not merely a cost-saving policy but the starting point of a patient-centered system reform.
Recently, the Ministry of Health and Welfare finalized a plan to lower the price calculation rate for generics and off-patent medicines from 53.55% to 45%. At the same time, it established a structure that provides pricing incentives for innovative and quasi-innovative pharmaceutical companies with high levels of R&D investment.
Through this, the government aims to improve the generic-centered market structure and encourage a transition toward an R&D-driven industry.
One industry official explained, “This reform has more of the character of industrial restructuring than a simple drug price reduction policy. The expectation is that companies with insufficient R&D investment will naturally lose competitiveness, while the industry is reorganized around companies with strong innovative drug development capabilities.”
Another industry official said, “It is important to create a virtuous cycle in which the financial resources secured through price reductions are reinvested into innovative medicines and R&D. If only the cost-saving effect is emphasized but does not lead to actual improvements in access, the justification for the reform could weaken.”
In other words, the financial resources secured through drug price reductions should not merely remain as industry support but should be directed toward areas that the public can directly benefit from, such as improved access to innovative medicines and strengthened stability of essential medicine supply.
RSA Expansion and flexible pricing agreements… Can they improve patient access?
Experts are turning their attention to the expansion of risk-sharing agreements (RSA) and more flexible drug pricing contracts.
A risk-sharing agreement allows the government and pharmaceutical companies to share the financial burden associated with high-cost innovative drugs. In Korea, many oncology drugs and rare disease treatments have already entered the reimbursement system through this mechanism.
However, experts believe that the current refund-based RSA model alone has limitations.
One industry official said, “The current structure tries to complete almost all evaluations before a drug enters the reimbursement system. As a result, patients wait longer, and the system spends a great deal of time trying to reduce uncertainty.”
The official continued, “A more realistic approach may be to embrace a certain level of uncertainty, secure patient access first, and then evaluate effectiveness using real-world data before adjusting the drug price. Going forward, post-listing management is likely to become more important than pre-listing review.”
Discussions are also continuing regarding evaluation criteria in terms of clinical usefulness. In the past, overall survival (OS) was considered the most important clinical endpoint. More recently, however, there have been increasing calls to consider a broader range of values, including long-term survival, recurrence prevention, and improvements in quality of life.
In fact, many innovative new drugs have demonstrated the potential for long-term survival benefits even before mature OS data become available, through improvements in progression-free survival (PFS), positive trends in PFS2, and invasive disease-free survival (iDFS).
One medical oncologist said, “OS remains an important endpoint in solid tumors, but in the current oncology treatment environment, it is often difficult to explain all of a therapy’s value using OS alone. As the number of long-term survivors increases and subsequent treatment options become more diverse, interpreting OS itself has become more complex than in the past.”
The physician continued, “Difficult-to-treat cancers and rare cancers have small patient populations and poor prognoses, rendering generating OS data difficult. If OS is applied as an absolute standard without considering disease characteristics and unmet medical needs, patients may have to wait even longer before gaining access to new treatment opportunities.”
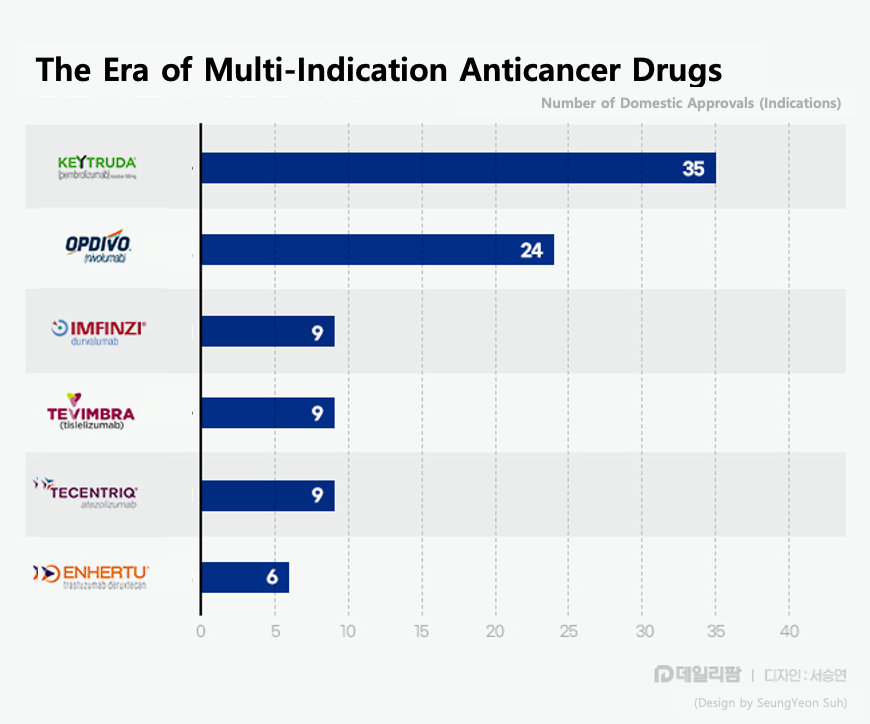
Recently, there have also been calls for greater flexibility in the existing reimbursement system, particularly for immuno-oncology drugs and antibody-drug conjugates (ADCs), where indication expansion is occurring rapidly. For example, Keytruda currently has 35 approved indications in Korea alone. In effect, a single product is functioning as dozens of different therapies.
The problem is that reimbursement reviews are repeated every time a new indication is added. If one indication remains under discussion at the CDDC or DREC stage for an extended period, subsequent indications must wait their turn for review. As the gap between the pace of innovative new drug development and the pace of reimbursement review widens, patient access issues are likely to persist.
This is also why the Korean Research-based Pharmaceutical Industry Association (KRPIA) has advocated the introduction of Indication-Based Pricing (IBP). Under the current system, a drug is reimbursed at the same price regardless of how many indications it has. In practice, however, treatment effectiveness, patient population size, and cost-effectiveness of a single drug can vary significantly by indication.
Recently, there have also been calls to expand beyond simple refund-based agreements and adopt outcome-based risk-sharing agreements. At present, most RSA arrangements in Korea are based on claims refunds or expenditure caps. Overseas, however, outcome-based agreements, in which pharmaceutical companies bear part of the cost if real-world treatment outcomes fail to meet expectations, are becoming the trend.
Ultimately, discussions surrounding reimbursement for innovative oncology drugs are not simply about adjusting drug prices. The key challenge going forward will be whether the system can adequately reflect emerging treatment values, including extended survival, the possibility of cure, and improved patient access.
One industry official emphasized, “In the past, the most important issue was whether a new drug received regulatory approval. Today, the more important question is how quickly patients can actually benefit from treatment. The reimbursement system also needs to evolve in a direction that improves flexibility and predictability in line with changes in the treatment environment.”
-

- 0
댓글 운영방식은
댓글은 실명게재와 익명게재 방식이 있으며, 실명은 이름과 아이디가 노출됩니다. 익명은 필명으로 등록 가능하며, 대댓글은 익명으로 등록 가능합니다.
댓글 노출방식은
댓글 명예자문위원(팜-코니언-필기모양 아이콘)으로 위촉된 데일리팜 회원의 댓글은 ‘게시판형 보기’와 ’펼쳐보기형’ 리스트에서 항상 최상단에 노출됩니다. 새로운 댓글을 올리는 일반회원은 ‘게시판형’과 ‘펼쳐보기형’ 모두 팜코니언 회원이 쓴 댓글의 하단에 실시간 노출됩니다.
댓글의 삭제 기준은
다음의 경우 사전 통보없이 삭제하고 아이디 이용정지 또는 영구 가입제한이 될 수도 있습니다.
-
저작권·인격권 등 타인의 권리를 침해하는 경우
상용 프로그램의 등록과 게재, 배포를 안내하는 게시물
타인 또는 제3자의 저작권 및 기타 권리를 침해한 내용을 담은 게시물
-
근거 없는 비방·명예를 훼손하는 게시물
특정 이용자 및 개인에 대한 인신 공격적인 내용의 글 및 직접적인 욕설이 사용된 경우
특정 지역 및 종교간의 감정대립을 조장하는 내용
사실 확인이 안된 소문을 유포 시키는 경우
욕설과 비어, 속어를 담은 내용
정당법 및 공직선거법, 관계 법령에 저촉되는 경우(선관위 요청 시 즉시 삭제)
특정 지역이나 단체를 비하하는 경우
특정인의 명예를 훼손하여 해당인이 삭제를 요청하는 경우
특정인의 개인정보(주민등록번호, 전화, 상세주소 등)를 무단으로 게시하는 경우
타인의 ID 혹은 닉네임을 도용하는 경우
-
게시판 특성상 제한되는 내용
서비스 주제와 맞지 않는 내용의 글을 게재한 경우
동일 내용의 연속 게재 및 여러 기사에 중복 게재한 경우
부분적으로 변경하여 반복 게재하는 경우도 포함
제목과 관련 없는 내용의 게시물, 제목과 본문이 무관한 경우
돈벌기 및 직·간접 상업적 목적의 내용이 포함된 게시물
게시물 읽기 유도 등을 위해 내용과 무관한 제목을 사용한 경우
-
수사기관 등의 공식적인 요청이 있는 경우
-
기타사항
각 서비스의 필요성에 따라 미리 공지한 경우
기타 법률에 저촉되는 정보 게재를 목적으로 할 경우
기타 원만한 운영을 위해 운영자가 필요하다고 판단되는 내용
-
사실 관계 확인 후 삭제
저작권자로부터 허락받지 않은 내용을 무단 게재, 복제, 배포하는 경우
타인의 초상권을 침해하거나 개인정보를 유출하는 경우
당사에 제공한 이용자의 정보가 허위인 경우 (타인의 ID, 비밀번호 도용 등)
※이상의 내용중 일부 사항에 적용될 경우 이용약관 및 관련 법률에 의해 제재를 받으실 수도 있으며, 민·형사상 처벌을 받을 수도 있습니다.
※위에 명시되지 않은 내용이더라도 불법적인 내용으로 판단되거나 데일리팜 서비스에 바람직하지 않다고 판단되는 경우는 선 조치 이후 본 관리 기준을 수정 공시하겠습니다.
※기타 문의 사항은 데일리팜 운영자에게 연락주십시오. 메일 주소는 dailypharm@dailypharm.com입니다.